Note: This report is so damning of the mental health system, they do not want you to see the report. You can go to the King County mental health website and you will not see this report. You had to know it exists and ask for it. Reports for the first two years are posted on this website.
SUMMARY OF WELLNESS ORDINANCE THAT SHOWS LACK OF “WELLNESS”
Outcomes in King County – The Recovery Ordinance Reports

King County prefers to use what they call their “Report Cards” and these show similar poor results.
Outcomes – Psychiatric Symptoms – King County’s Year End Report Cards reveal a six year trend of an increasing number of clients having worse symptoms or no change in symptoms after a year of services.
Note: The psychiatric symptoms measure was removed from the report card in 2006 so you can no longer track symptoms this way.

King County Outcomes – Level of Functioning
The Global Assessment of Functioning (GAF) is a numeric scale (0 through 100) used by mental health clinicians and physicians to rate subjectively the social, occupational, and psychological functioning of adults, e.g., how well or adaptively one is meeting various problems-in-living. The scale is presented and described in the DSM-IV-TR on page 34. The score is often given as a range, as outlined below:
- 91 – 100 No symptoms. Superior functioning in a wide range of activities, life’s problems never seem to get out of hand, is sought out by others because of his or her many positive qualities.
- 81 – 90 Absent or minimal symptoms (e.g., mild anxiety before an exam), good functioning in all areas, interested and involved in a wide range of activities, socially effective, generally satisfied with life, no more than everyday problems or concerns (e.g., an occasional argument with family members).
- 71 – 80 If symptoms are present, they are transient and expectable reactions to psychosocial stressors (e.g., difficulty concentrating after family argument); no more than slight impairment in social, occupational, or school functioning (e.g., temporarily falling behind in schoolwork).
- 61 – 70 Some mild symptoms (e.g., depressed mood and mild insomnia) OR some difficulty in social, occupational, or school functioning (e.g., occasional truancy, or theft within the household), but generally functioning pretty well, has some meaningful interpersonal relationships.
- 51 – 60 Moderate symptoms (e.g., flat affect and circumstantial speech, occasional panic attacks) OR moderate difficulty in social, occupational, or school functioning (e.g., few friends, conflicts with peers or co-workers).
- 41 – 50 Serious symptoms (e.g., suicidal ideation, severe obsessional rituals, frequent shoplifting) OR any serious impairment in social, occupational, or school functioning (e.g., no friends, unable to keep a job).
- 31 – 40 Some impairment in reality testing or communication (e.g., speech is at times illogical, obscure, or irrelevant) OR major impairment in several areas, such as work or school, family relations, judgment, thinking, or mood (e.g., depressed adult avoids friends, neglects family, and is unable to work; child frequently beats up younger children, is defiant at home, and is failing at school).
- 21 – 30 Behavior is considerably influenced by delusions or hallucinations OR serious impairment, in communication or judgment (e.g., sometimes incoherent, acts grossly inappropriately, suicidal preoccupation) OR inability to function in almost all areas (e.g., stays in bed all day, no job, home, or friends)
- 11 – 20 Some danger of hurting self or others (e.g., suicide attempts without clear expectation of death; frequently violent; manic excitement) OR occasionally fails to maintain minimal personal hygiene (e.g., smears feces) OR gross impairment in communication (e.g., largely incoherent or mute).
- 1 – 10 Persistent danger of severely hurting self or others (e.g., recurrent violence) OR persistent inability to maintain minimal personal hygiene OR serious suicidal act with clear expectation of death.
- 0 Inadequate information
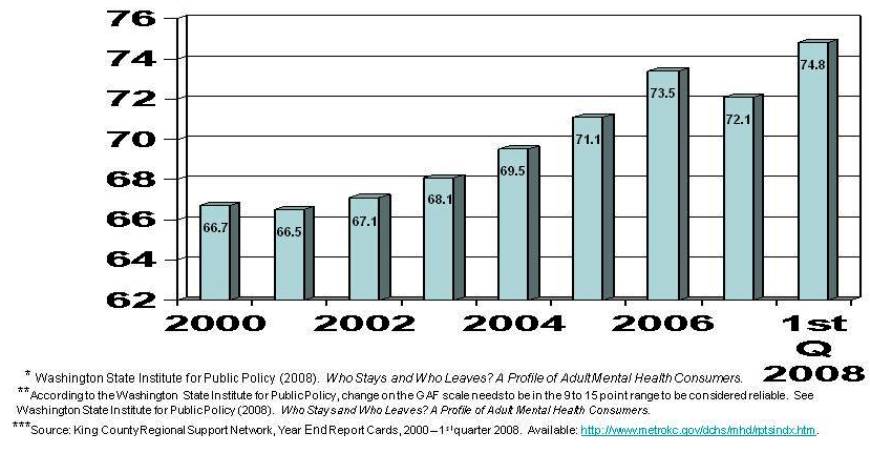
King County – Level of functioning further defined
This graph table shows you the GAF score, the where the clients are on this scale the the average change they experienced.

KING COUNTY DEPARTMENT OF COMMUNITY AND HUMAN SERVICES
Mental Health, Chemical Abuse and Dependency Services Division
King County Ordinance #13974
Second Annual Report: Recovery Model
BACKGROUND
The Metropolitan King County Council passed Ordinance #13974 on October 16, 2000. This ordinance is designed to promote recovery as an achievable outcome for adult consumers of the publicly funded mental health system in King County. The ordinance recognized that recovery is both a treatment philosophy and a process characterized by consumers moving toward participation in age-appropriate roles, including living independently, working, and having less dependence on the mental health system.
The ordinance required the Mental Health, Chemical Abuse and Dependency Services Division (MHCADSD) to submit:
A report in April 2001 that described steps the Division would take in redirecting the system toward recovery outcomes A written annual report to the Council that describes the performance of the mental health system toward achieving recovery outcomes, with calendar year 2001 as the evaluation baseline period.
This report addresses the second requirement.
…
“Ordinance # 12974 specifically required information about individuals who completed a benefit during the previous calendar year.”
…
Question 3 asks: By “recovery category”, how many consumers progressed, regressed, or remained unchanged.
7,009 clients began their benefit period as dependent. Of these:
6,433 (92%) remained dependent at the end of their benefit
573 (8%) progressed to less dependent
1 (<1%) progressed to recovered
2,295 clients began their benefit period as less dependent. Of these:
561 (24%) regressed
1,730 (75%) remained unchanged
4 (<1%) progressed to recovered
Overall, of the 9,304 consumers:
561 (6%) regressed
8,163 (88%) remained unchanged
580 (6%) progressed
CONCLUSIONS
Ultimately the success of a recovery-based model of care can only be assured through full commitment and participation by all stakeholders. Each must embody the belief that persons with mental illness can and will recover if necessary individualized supports are available to them. Although the publicly funded mental health system in King County – and across the United States – is stressed due to reductions in budgets that fund mental health services, the system must still strive to build a culture focused on principles of recovery. Over the past year MHCADSD has worked to build the foundation for a recovery model through the initiatives described above. The level of participation and support from stakeholders clearly shows that this is a shared vision and effort.
Note: You have to interpret the data in order to catch what they are not saying.
Of the 9,302 people – after a year of services:
75 % were dependent
88% were unchanged
8% became less dependent
less than 1% recovered – 5 people out of 9,302 in a year – after receiving their recommended treatment. This is actually half of half a percent.
If you go to the King County MH web page, you won’t even see mention of the 2001 Ordinance! The report and reporting requirements were all changed, including the definition of recovery.
Check their page here: ttp://www.kingcounty.gov/healthservices/MentalHealth/Recovery/KcMentalHealth/MHRecoveryPlan.aspx
In 2000 the King County Council passed the “Recovery Ordinance” which made progress toward recovery a central goal of the mental health system. In 2004, a Recovery Initiatives Committee was formed under the King County Mental Health, Chemical Abuse and Dependency Services Division (MHCADSD). In September 2005, the Division presented its “Recovery Plan for Mental Health Services” to the Metropolitan King County Council and in November of that year the Council passed an ordinance “adopting the recovery model as the policy framework for developing and operating the mental health services for which King County is responsible….” (Metropolitan King County Council, 2005, p.1)
However, despite its outward support of the recovery model, the King County system’s own outcome reports and publications, as well as additional information obtained through public disclosure requests, suggest that its primary goal, what it strives to achieve, is not recovery but warehousing. To borrow the language of the NFC, the King County mental health system is managing symptoms and accepting long term disability.
Outcomes in the King County system are revealed in three different sets of documents: the mental health division’s Year End Report Cards, the division’s Recovery Ordinance reports from 2001-2003, and data obtained through public disclosure requests. These sources point to a mental health system in which warehousing, rather than recovery, is the operational principal that determines how success and failure are measured. Warehousing is not just the outcome of current mental health services in King County. It is the mental health system’s guiding purpose.
